|
Background
Follow-up practices vary amongst hand surgeons and are not always patient-centred or resource efficient. Sometimes, patients attend costly in-person clinic appointments because they might have an issue to address, rather than because they do. Necessary appointments are not always timed to meet the patient’s needs, for example as soon as symptoms start to recur following a steroid injection, when a tendon repair fails, or when a Dupuytren’s contracture starts to interfere with daily activities. Some surgeons practise patient-initiated follow-up, but others argue that patients who would benefit from ongoing care can become lost to health services with this approach.
Patients given unnecessary appointments may not attend. In 2021/2022, 103 million outpatient appointments were missed across the NHS, costing the taxpayer an estimated £12.4 billion1,2. Conversely, patients may be unable to attend appointments which they need. People with financial difficulties, caring commitments, mental health problems, addictions, disabilities, language barriers, or low levels of health literacy may all struggle to attend appointments. After hand surgery, these groups, particularly, may end up with issues that go undiagnosed and untreated. The ideal follow-up strategy would identify all patients who have a clinical problem, as it occurs, without scheduling patients unnecessarily.
One approach to this is remote symptom monitoring via smartphone applications, which have a high and increasing uptake, even in disadvantaged groups3. By recording daily symptom severity, for example postoperatively, we can monitor whether a patient is recovering as expected. If the patient reports resolution of symptoms, they may not need an in-person appointment. When a patient experiences an unexpected deterioration in symptoms, this could be flagged and actioned early. Where eventual deterioration may be likely or expected (for example following steroid injection or percutaneous needle fasciotomy), clinic appointments could be scheduled based on symptom progression. Clinical problems in underserved groups could be identified and addressed.
This approach has had success in other fields. A recent trial in metastatic lung cancer was stopped early on ethical grounds because the survival advantage of remote symptom monitoring vs routine surveillance was so high (HR 0.59, [0.37; 0.96], p = 0.03)4. Advances in patient-reported outcome measures (PROMs) driven by BSSH5, and the increasing penetrance of smartphones amongst disadvantaged groups3 mean that we are nearly ready to trial this in UK hand surgery.
We have already shown that through novel PROM systems it is possible to monitor symptom severity in patients with base of thumb osteoarthritis or recent hand trauma, daily, for 12 weeks, with a 93% response rate6 (Figure 1).
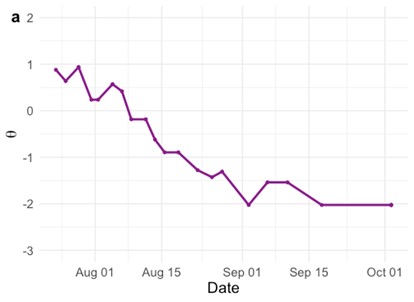
Figure 1. The recovery of a patient with a hand injury, captured via the EMCAT remote PROM monitoring platform6. Higher scores indicate more severe hand symptoms, a score of -2 is equivalent to normal hand function.
Recovery trajectories could be reviewed remotely and used to make decisions about the type and timing of follow-up. For example, the patient in Figure 1 has had complete resolution of symptoms and may not require a face-to-face appointment.
Our goal is to secure NIHR Health and Social Care Delivery Research (HSDR) funding to support a trial of remote monitoring vs standard care following common hand procedures such as carpal tunnel decompression, or steroid injection. We predict that patient-centred follow-up, guided by remote symptom monitoring, offers service efficiency gains, a reduction in missed appointments, earlier detection of complications, higher patient satisfaction, and a cost-benefit
References
1. NHS England. Reducing did not attends (DNAs) in outpatient services. Published 2023. Accessed July 7, 2023. https://www.england.nhs.uk/long-read/reducing-did-not-attends-dnas-in-outpatient-services/
2. NHS England. NHS to trial tech to cut missed appointments and save up to £20 million. Published 2018. Accessed July 7, 2023. https://www.england.nhs.uk/2018/10/nhs-to-trial-tech-to-cut-missed-appointments-and-save-up-to-20-million/#:~:text=With%20each%20hospital%20outpatient%20appointment,is%20coming%20to%20the%20NHS.
3. Honeyman M, Maguire D, Evans H, Davies A. Digital technology and health inequalities: a scoping review. Published 2020. Accessed July 7, 2023. https://phw.nhs.wales/publications/publications1/digital-technology-and-health-inequalities-a-scoping-review/
4. Denis F, Basch E, Septans AL, et al. Two-Year Survival Comparing Web-Based Symptom Monitoring vs Routine Surveillance Following Treatment for Lung Cancer. JAMA. 2019;321(3):306. doi:10.1001/jama.2018.18085
5. Kamran R, Rodrigues JN, Dobbs TD, Wormald JCR, Trickett RW, Harrison CJ. Computerized adaptive testing of symptom severity: a registry-based study of 924 patients with trapeziometacarpal arthritis. J Hand Surg Eur Vol. 2022;47(9):893-898. doi:10.1177/17531934221087572
6. Harrison C, Trickett R, Wormald J, et al. Remote Symptom Monitoring with Ecological Momentary Computerized Adaptive Testing (EMCAT): A Platform for Frequent, Low-Burden and Personalized Patient-Reported Outcome Measures (Preprint). Journal of Medical Internet Research; 2023. doi:10.2196/preprints.47179
|